Avicenna J Care Health Oper Room. 3(2):65-73.
doi: 10.34172/ajchor.102
Original Article
Presenting the Cognitive-Behavioral Exclusion Experience Model in the Field of Nursing
Davood Rahimishad Conceptualization, Data curation, Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing, 1 
Saeed Baghersalimi Conceptualization, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, *
Mohammadreza Azadehdel Formal analysis, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing, 1
Ruhollah Alikhan Gorgani Formal analysis, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing, 1
Author information:
1Department of Public Administration, Ra.C., Islamic Azad University, Rasht, Iran
Abstract
Background: Workplace ostracism refers to the experience of being excluded or ignored by colleagues or the organization, often leading to a range of negative consequences. This experience can have long-lasting psychological, behavioral, and organizational impacts. Accordingly, this study aimed to design and validate a strategic causal model of workplace ostracism experience among nurses.
Methods: A mixed-methods approach was employed to investigate the antecedents and consequences of workplace ostracism among nurses from 2023 to 2024. The population of the qualitative phase consisted of 12 academic experts and experienced nurses selected through purposive sampling. Data collection involved in-depth interviews and empirical experience analysis to identify the mechanisms and processes underlying nurses’ experience of ostracism. Thematic analysis was conducted using ATLAS.TI 8. Based on qualitative findings, a proposed model was developed and assessed in the quantitative phase. The quantitative sample included 400 nurses working in public hospitals in Qazvin, selected via random sampling and based on Morgan’s table. A validated researcher-made questionnaire was used for data collection. Eventually, confirmatory factor analysis (CFA) and path analysis were performed using AMOS 24.
Results: Qualitative findings indicated that workplace ostracism among nurses is influenced by high workload, lack of social support, non-transparent managerial decision-making, psychosocial stressors, and lack of professional advancement. In addition, the experience of ostracism was found to result in organizational silence, decreased motivation, social isolation, and decreased quality of patient care. Quantitative results revealed that path coefficients exceeded 0.7, and t-values were higher than 1.96, thus confirming the validity of the qualitative model and its overall reliability.
Conclusion: Overall, managing workplace ostracism experiences through fostering a supportive organizational culture, enhancing communication and conflict resolution skills, and improving work conditions can mitigate their negative effects among nurses. The proposed model provides a comprehensive framework for understanding the cognitive-behavioral dimensions of workplace ostracism and offers practical strategies for improving nurses’ work environments and enhancing human resource productivity in healthcare systems.
Keywords: Workplace ostracism, Cognitive-behavioral ostracism, Nurses, Experience management, Healthcare system
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Rahimishad D, Baghersalimi S, Azadehdel M, Alikhan Gorgani R. Presenting the cognitive-behavioral exclusion experience model in the field of nursing. Avicenna J Care Health Oper Room. 2025;3(2):65-73. doi:10.34172/ajchor.102
Introduction
Ostracism in nursing can be defined as the exclusion or dismissal of a nurse from the workplace due to inappropriate performance, rule violation, or misalignment with organizational values and goals. This experience can have serious psychological and professional consequences for the ostracized nurse and may negatively influence the quality of healthcare services (1,2). In addition, it can have significant adverse effects on mental health, job performance, and even social behavior (3). In workplace settings, ostracism manifests in various forms, such as being left out of group decisions, not being invited to meetings or social activities, and being ignored by colleagues (4). Research indicates that a large number of employees have experienced workplace ostracism, and its effects and consequences should not be overlooked accordingly (5).
This phenomenon can be influenced by a variety of cultural, social, and organizational factors (6). Ostracism not only undermines employees’ self-esteem and mental health but also threatens interpersonal relationships, productivity, and job commitment (7). Behavioral responses to this experience can range from passive withdrawal to acts of anger and retaliation (8). In some cases, even the mere perception of being at risk of exclusion or victimization can trigger intense emotional and psychological reactions (9).
Workplace ostracism is often described as “cold violence”, as it typically occurs covertly, making it difficult to monitor or control. Moreover, formal penalties are rarely associated with ostracizing behaviors (10). Unlike other forms of destructive workplace behaviors that may be overt, ostracism tends to be subtle and hidden, probably leading to more profound and long-lasting psychological consequences for employees (11). Individuals who are ostracized in organizational settings often develop gradual tendencies toward counterproductive workplace behaviors, whether overt or covert (12). These behaviors primarily contribute to organizational dysfunction, increased employee turnover, decreased productivity, and both direct and indirect organizational costs (13).
Cognitive and behavioral dimensions are crucial to the study of ostracism (14). The cognitive dimension pertains to an individual’s perceptions, beliefs, and emotions related to being excluded from work, while the behavioral dimension refers to observable actions that result from this experience (15). An individual may feel ostracized based solely on personal interpretation, or may be subjected to concrete behaviors that reinforce exclusion (16), both of which can lead to compensatory or even destructive reactions directed toward the organization (17).
The intensity and depth of ostracism among nurses and healthcare staff increased in the healthcare sector, especially during the coronavirus disease 19 pandemic (18). Nurses not only endured heavy workloads and psychological strain, but in some cases, experienced feelings of worthlessness or disposability due to employment conditions or managerial policies (19). The consequences of such ostracism included increased demotivation, intention to leave the profession, and decreased quality of healthcare services (20).
Therefore, supporting staff, particularly nurses—both psychologically and structurally within the organization—is essential for mitigating the damaging effects of ostracism while ensuring improved productivity and organizational performance (21). Despite the importance of this issue, domestic research has primarily focused on the quantitative analyses of ostracism, with limited attention to its deeper cognitive and behavioral aspects, or the practical and theoretical management of ostracism experiences (22).
For instance, El‐Sayed et al investigated the mediating role of organizational silence in the relationship between workplace ostracism and procrastination behaviors among nurses and observed that organizational silence considerably mediates and intensifies the negative effects of ostracism on procrastination. In other words, they found that nurses who experience ostracism and feel unable to express their concerns tend to display more procrastination behaviors, ultimately leading to reduced quality of care (1).
Similarly, Elliethey et al explored the relationship between work ethics, workplace ostracism, and counterproductive service behaviors among nurses and concluded that a strong work ethic serves as a protective factor, buffering against the detrimental effects of ostracism and reducing antiservice behaviors. Based on their findings, ostracism was associated with increased absenteeism, reduced motivation, and lower organizational commitment. In addition, their structural model confirmed that higher levels of work ethics can mitigate the adverse effects of ostracism (23).
Likewise, Basuny et al examined the relationship between experiences of ostracism and nurses’ perceptions of irresponsible behaviors among colleagues and reported that higher levels of perceived ostracism were associated with more negative perceptions of colleagues’ responsibility and a greater likelihood of engaging in such behaviors themselves. They further indicated that these patterns had harmful consequences for team morale, interpersonal interactions, and the overall quality of nursing care (24).
Despite its profound psychological, behavioral, and professional implications, ostracism in the nursing profession remains an understudied phenomenon. While its importance for improving the psychological well-being and performance of nurses is evident, previous research has rarely addressed its causal mechanisms or strategic management.
Elksas et al evaluated the effects of workplace ostracism on nurses’ job performance and work alienation and found that ostracism significantly reduced job performance and thereby increased work alienation. In turn, work alienation was linked to intentions to leave the profession and decreased job satisfaction, which can have serious implications for healthcare systems. Their study emphasized the importance of preventing and managing ostracism in healthcare settings in order to maintain high performance among nurses (14).
Identified Gaps in the Literature
-
Lack of Comprehensive Strategic Causal Models: Most previous studies adopted descriptive or fragmented approaches to workplace ostracism, neglecting strategic and causal perspectives. The present study addresses this gap by offering a structured causal model that identifies key variables and analyzes their interrelationships from a strategic standpoint.
-
Limited Context-Specific Research in Nursing: Much of the existing literature is rooted in general psychology or other occupational groups, with insufficient focus on nursing within its unique professional and cultural context. However, this study specifically centers on Iranian nurses, enhancing the relevance and applicability of findings in local healthcare environments.
-
Deficiency in Identifying Effective Coping and Preventive Strategies: Prior studies extensively focused on the experience of ostracism itself, with little attention to the development of practical coping mechanisms. This research contributes to this issue by defining and explaining scientifically grounded strategies based on a causal model that can effectively reduce ostracism while improving nurses’ performance.
-
Absence of Integrated Mixed-Method Analyses: Most prior research employed either purely qualitative or quantitative methodologies, lacking a holistic view. However, the current study adopts a mixed-methods approach to produce richer data and a more comprehensive understanding of the causal structure of workplace ostracism.
Accordingly, the main research question of this study is as follows:
What is the strategic causal model for managing workplace ostracism among nurses, and is it valid?
This approach not only provides deeper insights for researchers but also offers practical guidance for healthcare managers and decision-makers. By improving organizational relationships and psychological support systems, it is possible to prevent or mitigate ostracism and its destructive consequences in healthcare environments.
Methods
Study Design
This study employed a research method based on Saunders’ Research Onion Model, which encompasses multiple layers from research philosophy to data collection and analysis techniques. This model provides a systematic framework for advancing research processes. Moreover, the current study followed a mixed-methods (qualitative–quantitative) design to achieve its primary objective, utilizing complementary qualitative and quantitative phases (Figure 1).
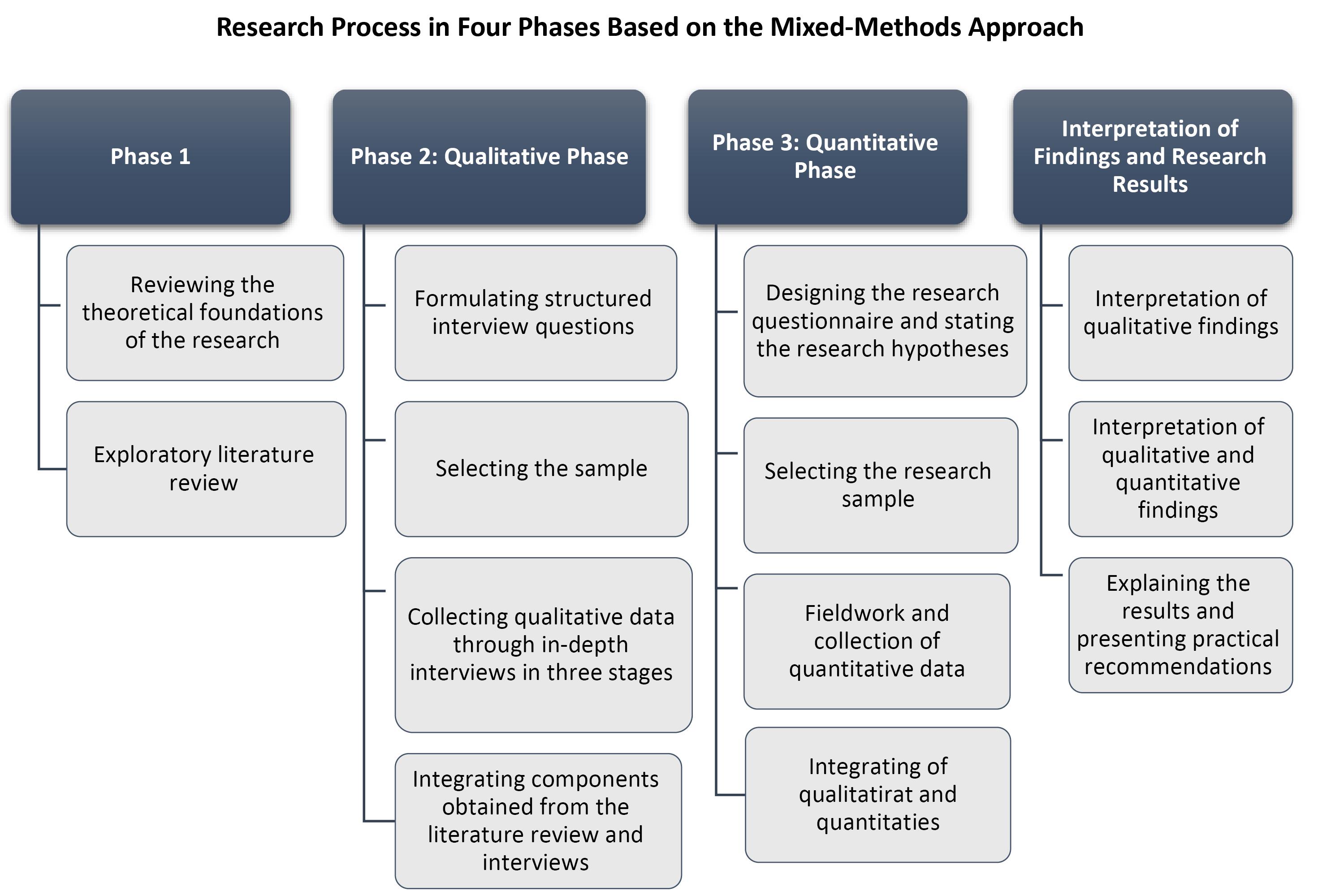
Figure 1.
Research Process
.
Research Process
Data Collection
Qualitative Phase
The qualitative phase was exploratory in nature and adopted an interpretivist philosophy with an inductive approach to identify and deeply understand the underlying components of ostracism. A single-case study strategy was applied in this section. The study population included academic experts and experienced nurses (N = 12) who had encountered workplace ostracism. Purposive sampling was used to select participants, and 12 semi-structured interviews were conducted with knowledgeable and relevant individuals. The interview process continued until theoretical saturation was reached and no new analytical insights were generated.
The primary data collection tool was a semi-structured interview guide, developed based on key and open-ended questions. It included three general questions, four questions targeting organizational factors, and three questions on strategic factors. Interviews were performed in Qazvin, and the face and content validity of the interview questions were evaluated by a panel of three nursing experts. Additionally, reliability and coding validation were ensured through performing test–retest on two interviews, with inter-coder agreement exceeding 80%, confirming coding consistency. Finally, qualitative data were analyzed using thematic analysis with the aid of ATLAS.ti software, version 8.
Quantitative Phase
The quantitative phase was conducted under a positivist philosophy with a deductive approach. The statistical population consisted of all nurses working in hospitals in Qazvin, and simple random sampling was performed using Morgan’s table. Based on Cochran’s formula, a sample of 400 nurses was selected from the available population. The main data collection instrument was a researcher-developed questionnaire, designed based on the themes and dimensions extracted from the qualitative phase. This questionnaire included general demographic questions, 18 items related to organizational factors, and 15 items addressing strategic factors.
Data Analysis
The validity of the questionnaire was evaluated through expert reviews in the fields of healthcare management and nursing. In addition, reliability was confirmed using Cronbach’s alpha coefficient, which exceeded 0.7, indicating acceptable internal consistency. Ultimately, quantitative data were analyzed using confirmatory factor analysis (CFA) with AMOS (version 24) and SPSS (version 24) software.
Ethical Considerations
Ethical considerations, which were of high importance in the qualitative phase, included respect for participants, protection of privacy, confidentiality of information, avoidance of bias, and accountability of the researcher. The researcher adhered to these ethical principles throughout the research process, including the design of the study, the collection and analysis of data, and the dissemination of findings.
Results
In this study, interviews were conducted with 12 participants, consisting of academic experts and experienced nurses who had encountered workplace ostracism, during the winter of 2024. Participants were categorized based on their educational level, work experience, and gender, and the corresponding frequencies and percentages are presented in Table 1.
Table 1.
Descriptive Statistics of the Study Participants
|
Variable
|
Category
|
Frequency (%)
|
| Gender |
Male |
7 (58) |
| Female |
5 (42) |
| Work experience |
5–10 years |
1 (9) |
| 11–20 years |
8 (64) |
| More than 20 years |
3 (27) |
| Education |
PhD and master’s degree |
5 (41) |
| Bachelor’s degree |
7 (59) |
According to the demographic data, the majority of the interviewees were male (58%), while females comprised 42% of the sample. Based on the results (Table 1), 9%, 64%, and 27% of the participants had 5–10, 11–20, and more than 20 years of work experience, respectively. In terms of educational level, 41% held doctoral or master’s degrees, and 59% had a bachelor’s degree.
The Process of Developing Sub-Categories, Themes, and Global Themes
Phase 1: Extraction of Initial Codes (Sub-Categories/Codes)
The process began with the analysis of semi-structured interviews or collected texts. Any phrase, sentence, or paragraph conveying a meaningful concept relevant to the phenomenon was assigned a code. Overall, 232 initial codes were extracted from the qualitative data.
Phase 2: Formation of Sub-Themes
Similar or related codes were grouped together under a common conceptual category, forming sub-themes. For example, codes such as “heavy workload”, “resource shortages”, and “lack of managerial support”, were classified under a sub-theme entitled “work environment challenges”.
Phase 3: Formation of Main Themes (Organizing Themes)
Sub-themes reflecting broader meanings and highlighting significant aspects of the phenomenon were clustered under main themes. For instance, sub-themes such as “organizational culture”, “management structure”, and “professional development opportunities” were categorized under the main theme of “internal organizational factors”.
Phase 4: Extraction of Global Themes (Conceptual Framework)
The main themes were synthesized into global themes, forming the overarching framework of the study. The global themes included (1) organizational and external factors (with 44 primary sub-themes) as the antecedents or foundations of workplace ostracism and (2) strategies and coping mechanisms for ostracism (with 34 primary sub-themes), detailing adaptive and preventive responses to the experience.
Theme Exploration
The thematic analysis process was conducted with the aim of uncovering the hidden and profound dimensions of rejection experiences among nurses. In this regard, following semi-structured interviews and initial coding, the data were categorized into three main organizing categories: “intra-organizational factors”, “extra-organizational factors”, and “coping strategies and mechanisms”. Subthemes (theme networks) for each extracted category were developed through the aggregation of similar codes and content analysis of participant statements.
To enhance the credibility and transparency of the findings, selected verbatim excerpts (quotations) from participants are presented for each foundational theme, providing an authentic and objective depiction of nurses’ lived experiences of rejection and their coping strategies. Table 2 provides the identified theme networks, theme classifications, and examples of participant quotations.
Table 2.
Final Codes After Screening
|
Overarching category
|
Organizing category
|
Theme network (core theme)
|
Quotation (participant verbatim sample)
|
| Cognitive-behavioral model of nurses’ rejection experience |
Intra-organizational factors |
Organizational culture and policies |
“Here, all decisions are made behind closed doors; we are never informed.” (P2, female, 16 years of experience) |
| Workload and resources |
“The number of staff is really insufficient relative to the workload; sometimes, I work several shifts back-to-back without rest.” (P5, female, 12 years of experience) |
| Management and professional development |
“Nurses are rarely offered training or promotion opportunities.” (P8, male, 20 years of experience) |
| Extra-organizational factors |
Economic and social pressures |
“Economic conditions often prevent me from focusing on my job; financial concerns have increased.” (P10, female, 10 years of experience) |
| Macro policies of the health system |
“Macro-level plans and decisions are always physician-centered; nurses are viewed only as executors.” (P3, male, 18 years of experience) |
| Media influence and public perception |
“The media rarely portray the reality of our work; everyone thinks nurses are merely assistants to physicians.” (P6, female, 14 years of experience) |
| Coping strategies and mechanisms |
Strengthening of individual and psychological capabilities |
“I try to stay strong by studying and acquiring new skills.” (P4, female, 9 years of experience) |
| Strengthening of social relationships and support |
“I always try to maintain a network of colleagues to support and energize me.” (P7, male, 13 years of experience) |
| Improvement of work environment and organizational culture |
“To improve work culture, there must be an environment of respect among members, not blame or neglect.” (P1, male, 15 years of experience) |
| Stress management and mental health |
“Exercise and reading during leisure time help me reduce burnout and stress.” (P9, male, 17 years of experience) |
| Performance improvement and professional development |
“Without motivation for advancement and learning, nurses quickly become burned out.” (P12, male, 20 years of experience) |
Quantitative Section
In the quantitative phase, based on the collected data, 80% of the respondents were female and 20% were male. In terms of age distribution, 50.6% of the participants were between 25 and 35 years old, 24% were aged 36–45, 13.8% were between 46 and 50 years old, and 11.6% were over 50 years of age. Regarding educational background, 77.5% of the respondents held a bachelor’s degree, while 22.5% had a master’s degree or higher (Table 3).
Table 3.
Descriptive Statistics–Quantitative Section
|
Variable
|
Category
|
Frequency (%)
|
| Gender |
Male |
80 (20.0) |
| Female |
320 (80.0) |
| Age |
25–35 years |
201 (50.6) |
| 36–45 years |
91 (24.0) |
| 46–50 years |
55 (13.8) |
| Over 50 years |
46 (11.6) |
| Education |
Bachelor’s degree |
310 (77.5) |
| Master’s or higher |
90 (22.5) |
| Total sample |
|
400 (100) |
Confirmatory Factor Analysis of Macro-Level Organizational Variables (Causal Factors)
CFA was employed to determine the validity of macro-level organizational variables. The values along the paths represent factor loadings, all of which exceeded 0.60, indicating acceptable convergent validity.
The fit indices related to model evaluation (Table 4) demonstrate that indices such as comparative fit index (CFI), goodness of fit index (GFI), normed fit index (NFI), root mean square residual (RMR), and root mean square error of approximation (RMSEA) fall within acceptable thresholds. These goodness-of-fit indices indicate that the data of this study are appropriately fitted to the factor structure of the model, reflecting strong alignment between the items and the underlying construct of macro-level organizational factors.
Table 4.
Model Fit Indices for Macro-Level Organizational Variables
|
Index type
|
Fit index name
|
Abbreviation
|
Acceptable threshold
|
Value in this study
|
| Absolute fit |
Degrees of freedom |
DF |
– |
212 |
| Significance level |
P |
Less than 0.05 |
0.000 |
| Chi-square/degree of freedom ratio |
CMIN/DF |
Between 1 and 5 |
1.73 |
| Chi-square coverage level |
Chi-Square |
Above 5% |
0.4 |
| Comparative fit index |
CFI |
Greater than 0.90 |
0.934 |
| Adjusted goodness of fit index |
AGFI |
Greater than 0.90 |
0.940 |
| Comparative fit |
Non-normed fit index |
NNFI |
Greater than 0.90 |
0.92 |
| Normed fit index |
NFI |
Close to 1 |
0.93 |
| Comparative fit index |
CFI |
Greater than 0.90 |
0.934 |
| Relative fit index |
RFI |
Greater than 0.50 |
0.64 |
| Incremental fit index |
IFI |
Between 0 and 1 |
0.60 |
| Parsimonious fit |
Parsimonious normed fit index |
PNFI |
Greater than 0.50 |
0.75 |
| Parsimonious goodness-of-fit index |
PGFI |
Greater than 0.50 |
0.911 |
| Root mean square error of approximation |
RMSEA |
Less than 0.10 |
0.045 |
| Normalized chi-square |
CMIN |
Between 1 and 3 |
2.2 |
Confirmatory Factor Analysis of Coping Strategies and Mechanisms
CFA was conducted to assess the validity of coping strategies and mechanisms. The values on the paths represent factor loadings, all of which were above 0.60, confirming adequate convergent validity.
The model fit indices associated with the proposed coping strategies (Table 5) revealed that CFI, GFI, NFI, RMR, and RMSEA fall within acceptable thresholds. These goodness-of-fit indicators confirm that the data align well with the factor structure of the proposed model, suggesting a strong correspondence between the items and the latent construct of coping strategies. Figure 2 displays the path coefficient analysis of the model.
Table 5.
Model Fit Indices for Coping Strategies and Mechanisms
|
Index type
|
Fit index name
|
Abbreviation
|
Acceptable threshold
|
Value in this study
|
| Absolute fit |
Degrees of freedom |
DF |
– |
212 |
| Significance level |
P |
Less than 0.05 |
0.000 |
| Chi-square/degree of freedom ratio |
CMIN/DF |
Between 1 and 5 |
2.96 |
| Chi-square coverage level |
Chi-Square |
Greater than 5% |
0.14 |
| Comparative fit index |
CFI |
Greater than 0.90 |
0.955 |
| Adjusted goodness of fit index |
AGFI |
Greater than 0.90 |
0.941 |
| Comparative fit |
Non-normed fit index |
NNFI |
Greater than 0.90 |
0.90 |
| Normed fit index |
NFI |
Close to 1 |
0.99 |
| Comparative fit index |
CFI |
Greater than 0.90 |
0.955 |
| Relative fit index |
RFI |
Greater than 0.50 |
0.64 |
| Incremental fit index |
IFI |
Between 0 and 1 |
0.59 |
| Parsimonious fit |
Parsimonious normed fit index |
PNFI |
Greater than 0.50 |
0.99 |
| Parsimonious goodness-of-fit index |
PGFI |
Greater than 0.50 |
0.901 |
| Root mean square error of approximation |
RMSEA |
Less than 0.10 |
0.069 |
| Normalized chi-square |
CMIN |
Between 1 and 3 |
1.9 |
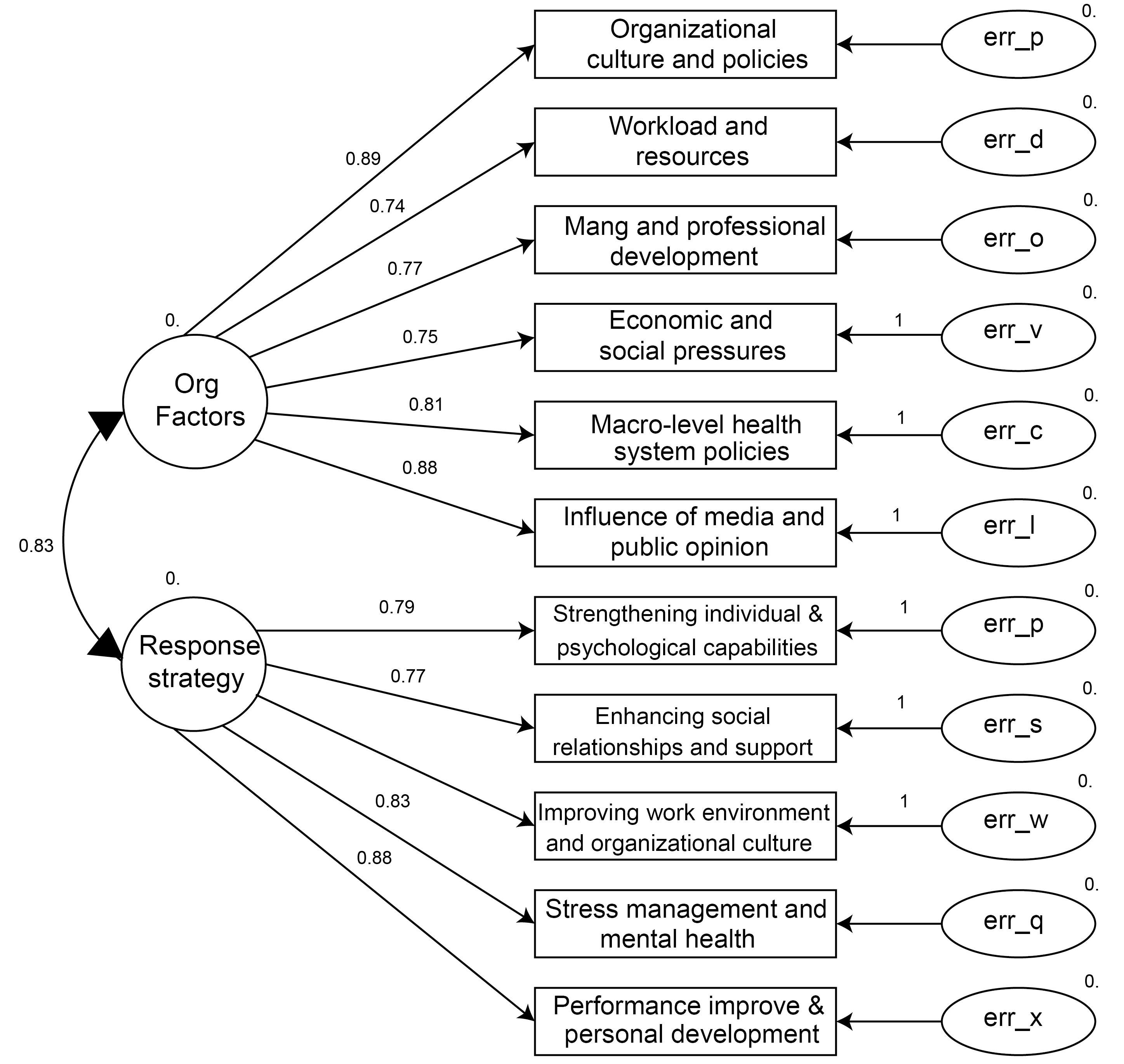
Figure 2.
The Path Coefficient Analysis of the Model
.
The Path Coefficient Analysis of the Model
Discussion
Rejection among nursing staff is a multidimensional phenomenon resulting from a combination of macro-level organizational factors, both internal and external to the organization. This experience is not simply limited to personal interactions or individual conflicts. These findings conform to those of the study by Basuny et al, highlighting limited personal interaction and lack of accountability among colleagues (24). At the intra-organizational level, the existence of a power-driven organizational culture, dominance of non-participatory policies, and structures that restrict nurses’ participation in decision-making play a significant role in intensifying feelings of rejection (5). This part of the results is consistent with the results of the research by Elliethey et al, demonstrating that experiences of rejection lead to increased negative behaviors, such as absenteeism, decreased motivation, and reduced organizational commitment (23).
This study also identified that high workload, lack of resources and facilities, insufficient opportunities for career growth and development, inappropriate management styles, and absence of effective training contribute to feelings of neglect, weakening capabilities, and ultimately the marginalization of nurses within the organizational structure. These results corroborate those of El-Sayed et al, pointing to the concurrent experience of rejection and inability to express problems (1).
Beyond these factors, external elements (e.g., economic pressures, excessive societal and familial expectations, top-down physician-centered policies in the health system, and neglect of nursing roles) subject nurses to injustice and feelings of worthlessness. Furthermore, stereotypical and inaccurate representations of the nursing profession in the media have led to a decline in the social status and symbolic experiences of rejection among nurses.
In response to these conditions, nurses are compelled to adopt a range of strategies encompassing individual, social, and organizational dimensions. At the individual level, efforts to enhance self-awareness, increase resilience, and learn and apply emotion management and coping skills play a vital role in psychological protection. In terms of social relationships, showing empathy and support among colleagues, families, and patients, forming support networks, and participating in empathetic groups are crucial in reducing feelings of isolation and rejection (10).
At the organizational level, pursuing professional demands through collective mechanisms, actively participating in meetings and decision-making, establishing constructive communication channels with managers, and striving to change the dominant organizational culture are important pathways for managing and alleviating rejection. These findings are in line with the results of the study by Elksas et al, showing that rejection experiences directly lead to reduced job performance, increased alienation from the work environment, and occupational isolation among nurses (14).
Stress management and mental health approaches, such as starting meditation, striving for quality sleep, doing exercise, and utilizing psychological services, are also highly effective in maintaining professional functioning and improving the quality of life for nurses (13). On the other hand, many nurses attempt to transform their experiences of rejection into positive motivation for further learning, professional development, knowledge enhancement, and demonstration of their competencies in the workplace (2,9).
Overall, the mentioned strategies—if supported by the health system’s structure—can not only reduce the intensity and negative consequences of rejection but also provide an opportunity for empowerment and the advancement of the professional status of nursing in society.
Conclusion
Our results indicated that rejection among nursing staff is a deep-rooted and multilayered phenomenon that does not stem solely from individual interactions but arises from the interplay between macro-level intra-organizational and extra-organizational factors. Feelings of rejection are intensified by several key factors, such as power-driven organizational culture and structures, workload pressures, weaknesses in career development pathways, physician-centered upstream policies, economic conditions, and inaccurate media representation of nursing. However, nurses can employ a number of strategies to mitigate the negative consequences of rejection, including enhancing individual and professional capabilities, creating and strengthening support networks, striving for greater participation in organizational decision-making, and caring for mental health. Therefore, effectively addressing rejection and empowering nurses require structural and cultural organizational reforms, supportive policy formulation, and media attention to the values of the nursing profession.
Recommendations Based on Organizational Factors
-
Redefining cultural components with an emphasis on strengthening the sense of belonging, mutual trust, organizational respect, and institutionalized behaviors based on transparency and justice in managerial decisions and interpersonal interactions.
-
Establishing dynamic workload management systems in order to prevent occupational overload, promote distributive justice, and reduce nurse burnout through developing clinical protocols and enhancing human resource capacities.
-
Designing and implementing career pathway maps, defining meritocratic criteria, and creating opportunities for continuous learning and development with the active participation of nurses in professional advancement programs.
-
Adopting macro-level, evidence-based policies aimed at enhancing nurses’ social status, job security, and professional welfare.
-
Conducting multimedia awareness campaigns in order to correct and enhance the public image of nursing, clarify nurses’ roles in the health system, and strengthen the social capital of these healthcare professionals nationally.
Recommendations Based on Major Strategies
-
Developing individual capacity-building programs, positive psychology-based instruments, and mindfulness techniques to increase nurses’ flexibility and resilience.
-
Creating peer support networks for sharing experience, strengthening solidarity, and providing psychosocial support among colleagues.
-
Institutionalizing mechanisms for the active participation of nurses in the process of policymaking and development of organizational protocols in order to amplify their voice and enhance their sense of professional impact.
Acknowledgments
The authors extend their deepest gratitude to all those who played a key role in conducting this research, especially the nurses who significantly contributed as participants in data collection. It is worth mentioning that this study was approved by the Ethics Committee OF Islamic Azad University (IR.IAU.LIAU.REC.1404.001).
This article has been extracted from the first author’s doctoral dissertation submitted to Islamic Azad University, Rasht Branch, Rasht, Iran.
Competing Interests
We have no conflict of interests to disclose.
Consent for Publication
Not applicable.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request. The entire dataset is in the Farsi language. Nonetheless, the data can be provided in English for readers upon reasonable request from the corresponding author.
Ethical Approval
This study was approved by the Ethics Committee of Islamic Azad University (IR.IAU.LIAU.REC.1404.001). This article has been extracted from the first author’s doctoral dissertation submitted to Islamic Azad University, Rasht Branch, Rasht, Iran. All study protocols were approved by the Ethics Committee of Islamic Azad University. In addition, all methods were performed in accordance with relevant guidelines and regulations.
Furthermore, participants or their legal guardians were provided with an information sheet, reassured about anonymity and data confidentiality, and free to withdraw from the study. Moreover, the purpose of the study was explained to participants/their legal guardians, and an informed consent form was obtained from them before starting the study.
Funding
Not applicable.
References
- El-Sayed AA, Ali MS, Abdel Razek NM, Abdelaliem SM, Asal MG. The effect of organizational silence on the relationship between workplace ostracism and nurses’ procrastination behavior: a structural equation modeling. Int Nurs Rev 2025; 72(2):e13050. doi: 10.1111/inr.13050 [Crossref] [ Google Scholar]
- Sharma N, Dhar RL. Workplace ostracism: a process model for coping and typologies for handling ostracism. Hum Resour Manag Rev 2024; 34(1):100990. doi: 10.1016/j.hrmr.2023.100990 [Crossref] [ Google Scholar]
- Omidi Moghadam E, Mojtabaei M, Ashori A, Khodabakhsh F, Rahmani E, Bayat Mazlaghani M. Comparing the effectiveness of short-term psychodynamic therapy with training in cognitive emotion regulation strategies on body dysmorphic symptoms and executive functions of people with health anxiety. Iranian Journal of Psychiatric Nursing 2025;13(2):113-26. [Persian].
- Huang W, Yuan C. Workplace ostracism and helping behavior: a cross-level investigation. J Bus Ethics 2024; 190(4):787-800. doi: 10.1007/s10551-023-05430-z [Crossref] [ Google Scholar]
- Ibrahim R, Olaleye BR. Relationship between workplace ostracism and job productivity: the mediating effect of emotional exhaustion and lack of motivation. Asia Pac J Bus Adm 2024; 17(1):190-211. doi: 10.1108/apjba-08-2023-0408 [Crossref] [ Google Scholar]
- Sharifzadeh M, Razeghi N, Aghaei H, Tabatabaee SM. The comparing effectiveness of emotion-focused therapy and mindfulness-based cognitive therapy on worry in patients with generalized anxiety disorder. Iranian Journal of Psychiatric Nursing 2025;13(2):101-12. [Persian].
- Ali Awad NH, Mohamed El Sayed BK. Post COVID-19 workplace ostracism and counterproductive behaviors: moral leadership. Nurs Ethics 2023; 30(7-8):990-1002. doi: 10.1177/09697330231169935 [Crossref] [ Google Scholar]
- Ali AZ, Alkubati SA, Pasay-An E, Alreshidi M, Alrashidi N, Alabonassir O. Investigating the level and predictors of nursing care quality and its correlation with workplace ostracism and innovative work behavior: approach for workplace and practical enhancement. BMC Nurs 2025; 24(1):541. doi: 10.1186/s12912-025-03200-y [Crossref] [ Google Scholar]
- Chang HY, Huang TL, Wong MK, Shyu YL, Ho LH, Chen LC. Relationship between psychological ownership of the nursing profession and turnover intention: a correlational survey among Taiwanese nurses. J Nurs Manag 2022; 30(7):2927-36. doi: 10.1111/jonm.13670 [Crossref] [ Google Scholar]
- Chang HY, Lee IC, Tai SI, Ng NY, Shiau WL, Yu WP. Professional engagement: connecting self-efficacy to actual turnover among hospital nurses. J Adv Nurs 2023; 79(12):4756-66. doi: 10.1111/jan.15737 [Crossref] [ Google Scholar]
- Chen Y, Li S. Relationship between workplace ostracism and unsafe behaviors: the mediating effect of psychological detachment and emotional exhaustion. Psychol Rep 2020; 123(2):488-516. doi: 10.1177/0033294118813892 [Crossref] [ Google Scholar]
- Cheng C, Ma J. Effect of workplace ostracism on employee initiative behaviour: a chained double mediation model. J Manag Psychol 2022; 37(8):765-78. doi: 10.1108/jmp-10-2021-0541 [Crossref] [ Google Scholar]
- Chu X, Zhang L, Li M. Nurses’ strengths use and turnover intention: the roles of job crafting and self-efficacy. J Adv Nurs 2022; 78(7):2075-84. doi: 10.1111/jan.15124 [Crossref] [ Google Scholar]
- Elksas EI, Aziz Mansy AM, Mohammed Aly SM, Elsayed Abdo BM. Workplace ostracism and its relationship with job performance and work alienation among staff nurses. Assiut Sci Nurs J 2024; 12(47):198-209. doi: 10.21608/asnj.2024.333371.1944 [Crossref] [ Google Scholar]
- Dash D, Farooq R, Upadhyay S. Linking workplace ostracism and knowledge hoarding via organizational climate: a review and research agenda. Int J Innov Sci 2022; 15(1):135-66. doi: 10.1108/ijis-05-2021-0080 [Crossref] [ Google Scholar]
- Du S, Ma Y, Lee JY. Workplace loneliness and the need to belong in the era of COVID-19. Sustainability 2022; 14(8):4788. doi: 10.3390/su14084788 [Crossref] [ Google Scholar]
- Jahanzeb S, Fatima T, Javed B, Giles JP. Can mindfulness overcome the effects of workplace ostracism on job performance?. J Soc Psychol 2020; 160(5):589-602. doi: 10.1080/00224545.2019.1707465 [Crossref] [ Google Scholar]
- Jarden RJ, Scott S, Rickard N, Long K, Burke S, Morrison M. Factors contributing to nurse resignation during COVID-19: a qualitative descriptive study. J Adv Nurs 2023; 79(7):2484-501. doi: 10.1111/jan.15596 [Crossref] [ Google Scholar]
- Jawahar IM, Bilal AR, Fatima T, Mohammed ZJ. Does organizational cronyism undermine social capital? Testing the mediating role of workplace ostracism and the moderating role of workplace incivility. Career Dev Int 2021; 26(5):657-77. doi: 10.1108/cdi-09-2020-0228 [Crossref] [ Google Scholar]
- Jiang H, Jiang X, Sun P, Li X. Coping with workplace ostracism: the roles of emotional exhaustion and resilience in deviant behavior. Manag Decis 2020; 59(2):358-71. doi: 10.1108/md-06-2019-0848 [Crossref] [ Google Scholar]
- Liu C, Li H, Li L. Examining the curvilinear relationship of job performance, supervisor ostracism, and turnover intentions. J Vocat Behav 2022; 138:103787. doi: 10.1016/j.jvb.2022.103787 [Crossref] [ Google Scholar]
- Liu M, Liu X, Muskat B, Leung XY, Liu S. Employees’ self-esteem in psychological contract: workplace ostracism and counterproductive behavior. Tour Rev 2023; 79(1):152-66. doi: 10.1108/tr-11-2022-0535 [Crossref] [ Google Scholar]
- Elliethey NS, Abou Hashish EA, Ahmed Mohamed Elbassal N. Work ethics and its relationship with workplace ostracism and counterproductive work behaviours among nurses: a structural equation model. BMC Nurs 2024; 23(1):126. doi: 10.1186/s12912-024-01785-4 [Crossref] [ Google Scholar]
- Basuny HF, Abd El-Rahman RM, Al Anwer Ashour HM. The relationship between workplace ostracism and nurses’ perception of counterproductive work behaviors. Int J Novel Res Healthc Nurs 2024; 11(1):1-16. doi: 10.5281/zenodo.10489628 [Crossref] [ Google Scholar]